
Terminal cleaning is defined as the comprehensive disinfection of a patient care room after discharge or transfer, designed to eliminate pathogens and prepare the space for the next occupant. This process goes far beyond routine janitorial work. It targets every surface in the room, including walls, ceilings, ventilation grilles, and equipment, not just the visibly soiled areas. Regulatory bodies including the CDC, The Joint Commission, and QUAD A have established standards that make this process a compliance requirement, not a best practice suggestion. For cleaning professionals and facility managers, understanding what is terminal cleaning means understanding the difference between a room that looks clean and one that is microbiologically safe.
What is terminal cleaning and why does it matter?
Terminal cleaning is the full environmental decontamination of a patient room after it has been vacated, targeting all surfaces to break the chain of infection. Routine cleaning addresses visible dirt and high-touch surfaces during a patient's stay. Terminal cleaning resets the entire room to a microbiological baseline before the next patient arrives.
The stakes are real. Pathogens like MRSA and C. difficile survive on surfaces for days or weeks. Contaminated environments spread these organisms directly to the next patient, making thorough decontamination a patient safety issue, not just a housekeeping task. Facilities that skip or rush this process face both clinical consequences and accreditation risk.

The term "terminal" comes from the idea of terminating the microbial lifecycle in that environment. The industry also uses the phrase "full room decontamination" interchangeably, though terminal cleaning remains the regulated term recognized by accrediting bodies. Facility managers should use the regulated term in all documentation to avoid confusion during audits.
When should terminal cleaning be performed?
Specific trigger events determine when a full decontamination is required. Terminal cleaning is triggered after patient discharge, the end of an isolation period, outbreak resolution, or the completion of post-construction activities in a clinical space. Each of these events signals that the room's microbial load may be elevated beyond what routine cleaning can address.
The most common triggers include:
- Patient discharge or transfer to another unit or facility
- End of contact, droplet, or airborne isolation precautions
- Resolution of a facility-wide or unit-level outbreak
- Post-construction or renovation work in or adjacent to patient care areas
- Discovery of a confirmed multi-drug-resistant organism in the room
Routine cleaning runs on a scheduled cycle regardless of patient status. Enhanced cleaning increases frequency or intensity during an active outbreak but does not cover all surfaces. Terminal cleaning is the only level that addresses the full room environment, including low-touch and hidden surfaces. Knowing which trigger applies determines which cleaning level your team deploys, and deploying the wrong level creates a compliance gap.
Pro Tip: Create a trigger event log at the unit level. When nursing staff document a discharge or isolation lift, that entry should automatically prompt an environmental services work order for terminal cleaning. Manual communication chains break down; a documented trigger system does not.
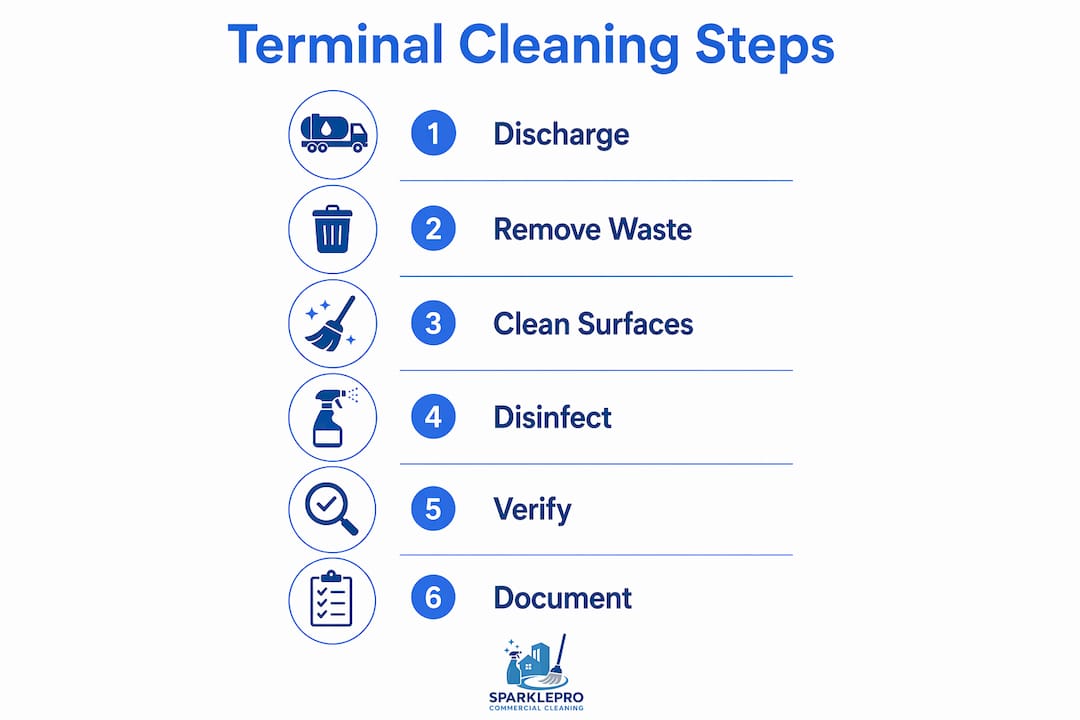
How to perform terminal cleaning: step-by-step procedures
Effective terminal cleaning follows a fixed sequence. Deviating from that sequence recontaminates already-cleaned surfaces and defeats the purpose of the process. The standard approach follows two rules: top to bottom, and clean to dirty.
- Don full PPE before entering. Gloves, gown, eye protection, and a mask are required. Proper PPE use protects staff and prevents cross-contamination from the cleaner's own clothing or hands.
- Remove all waste and linen. Bag and dispose of waste as medical waste. Strip all linen and place it in designated linen bags before any surface cleaning begins.
- Disassemble and remove portable equipment. Move IV poles, infusion pumps, and patient lifts out of the room for separate cleaning and drying before reassembly.
- Clean and disinfect from ceiling to floor. Start with ceiling vents and light fixtures, move to walls and window ledges, then work down to furniture, equipment, and finally the floor. This sequence prevents debris from falling onto already-cleaned surfaces.
- Apply an EPA-registered or TGA-registered disinfectant. Every surface requires disinfection with a product that carries an approved registration number. Apply at the manufacturer's specified concentration and allow the full contact time before wiping. Cutting contact time is the single most common compliance failure.
- Clean high-touch surfaces last within each zone. Light switches, call buttons, bed rails, and door handles carry the highest pathogen load. Clean them after the surrounding surfaces to avoid spreading contamination.
- Mop the floor using a clean mop head. Never reuse a mop head from a previous room. Work from the far corner toward the door.
- Complete the terminal cleaning checklist. Record the disinfectant product name, registration number, concentration, contact time, and the specific trigger event that prompted the clean. Sign and date the record.
Pro Tip: Use a UV-C verification device or ATP bioluminescence testing on a sample of surfaces after cleaning. These tools give you objective data on surface cleanliness and create a defensible quality record for accreditation surveys.
Refer to a disinfecting services guide to confirm that your chosen products meet current EPA registration requirements for the pathogens relevant to your facility type.
What documentation and regulatory standards apply?
Documentation is not optional in terminal cleaning. It is a regulatory requirement enforced during accreditation surveys. Completion records must include the disinfectant's product registration number, the concentration used, the contact time applied, and a direct link to the trigger event that prompted the clean. Retrospective or incomplete records are routinely rejected by auditors.
The key standards and bodies that govern this process include:
- The Joint Commission: Requires documented environmental cleaning protocols and trains surveyors to verify compliance through staff interviews, not just paperwork review.
- QUAD A: Applies terminal cleaning standards to ambulatory surgery centers and other outpatient settings, with surveyors specifically trained to assess EVS staff knowledge.
- CDC Guidelines for Environmental Infection Control: Provide the scientific basis for surface disinfection protocols, contact times, and product selection.
- NSQHS Standards (for Australian-aligned facilities): Require event-linked documentation and staff competency records for terminal cleaning procedures.
"The Joint Commission and QUAD A train surveyors to ask EVS staff to articulate their cleaning sequence during surveys. A staff member who cannot explain why they clean top to bottom, or why contact time matters, creates a citation risk for the facility regardless of what the paperwork shows."
The term "deep clean" appears frequently in commercial cleaning contracts. That term has no regulatory definition. Facilities that accept a commercial deep clean in place of a regulated terminal cleaning process are exposed during accreditation surveys. Accrediting bodies expect documented evidence of a specific, sequenced process tied to a named trigger event. A general deep clean does not satisfy that requirement.
Staff training is the compliance gap most facilities underestimate. Cleaning staff must be able to explain the logic of the cleaning sequence, not just execute it from memory. That understanding is what surveyors test.
How does terminal cleaning differ from routine and enhanced cleaning?
The three cleaning levels serve different purposes and are not interchangeable. Understanding the distinction prevents both under-cleaning and the misallocation of resources.
| Cleaning level | Trigger | Surface coverage | Regulatory threshold |
|---|---|---|---|
| Routine cleaning | Scheduled cycle | High-touch and visibly soiled surfaces | Standard janitorial compliance |
| Enhanced cleaning | Active outbreak or elevated risk | Increased frequency on high-touch surfaces | Outbreak response protocols |
| Terminal cleaning | Discharge, isolation end, outbreak resolution | All surfaces, full room decontamination | Joint Commission, QUAD A, CDC |
Terminal cleaning resets the room to a microbiological baseline. Routine cleaning maintains a baseline during occupancy. Enhanced cleaning slows transmission during an active event but does not achieve full decontamination. A facility that uses enhanced cleaning in place of terminal cleaning after a discharge is not meeting the regulatory standard, even if the room looks clean.
The practical implication for facility managers is clear. Each cleaning level requires a separate protocol, separate documentation, and separate staff training. Treating them as a single sliding scale of intensity is a compliance error.
Key Takeaways
Terminal cleaning is the only cleaning level that resets a patient room to a microbiological baseline, and it requires documented, trigger-linked evidence of a specific sequenced process to satisfy accreditation standards.
| Point | Details |
|---|---|
| Defined by trigger events | Terminal cleaning begins after discharge, isolation end, outbreak resolution, or post-construction work. |
| Full surface coverage required | Every surface, including ceilings, walls, and ventilation, must be cleaned and disinfected. |
| EPA-registered disinfectants only | Use products with approved registration numbers at specified concentrations and full contact times. |
| Documentation is a compliance requirement | Records must include product codes, concentrations, contact times, and the specific trigger event. |
| Staff must explain the sequence | Surveyors from The Joint Commission and QUAD A test staff knowledge, not just paperwork. |
What I've learned from watching facilities fail audits on terminal cleaning
The most consistent audit failure I see has nothing to do with the cleaning itself. Facilities invest in the right disinfectants, train staff on the sequence, and still get cited. The reason is almost always documentation that cannot be linked to a specific trigger event. A cleaning log that says "room 412 cleaned, october 14" tells a surveyor nothing. A log that says "room 412, terminal clean triggered by patient discharge, product X registration number Y, concentration Z, contact time 10 minutes, completed 14:32" tells them everything.
The second failure point is the gap between environmental services and clinical staff. Nursing teams lift isolation precautions and do not notify EVS. EVS completes a routine clean because no trigger was communicated. The room gets occupied again without a terminal clean on record. That sequence is a patient safety event and a citation waiting to happen. The fix is a formal handoff protocol, not a reminder email.
Training is the third gap. Facilities run staff through a procedure checklist once during onboarding and consider it done. Surveyors from The Joint Commission and QUAD A ask staff to explain why they follow the sequence they follow. A cleaner who says "because that's what the checklist says" fails that test. A cleaner who says "because cleaning top to bottom prevents recontamination of lower surfaces" passes it. That difference comes from training that explains the logic, not just the steps. Consistent cleaning standards, as outlined in health and safety guidance, require ongoing reinforcement, not one-time orientation.
— Sales
Sparkleprocommercialcleaning's approach to terminal cleaning compliance
Facility managers who need terminal cleaning that holds up under accreditation scrutiny require more than a cleaning crew with the right products. They need documented processes, trained staff, and audit-ready records tied to specific trigger events.
Sparkleprocommercialcleaning delivers terminal cleaning services built around regulatory compliance, with staff trained to execute and explain the full cleaning sequence. Services are available across Delaware, Massachusetts, Washington, and New Jersey, with documentation packages that satisfy Joint Commission and QUAD A survey requirements. Contact Sparkleprocommercialcleaning to schedule a site assessment and get a service quote aligned with your facility's compliance needs.
FAQ
What is the purpose of terminal cleaning?
Terminal cleaning eliminates pathogens from a patient room after discharge or isolation to prevent infection transmission to the next occupant. It resets the room to a microbiological baseline that routine cleaning cannot achieve.
What surfaces does terminal cleaning cover?
Terminal cleaning covers every surface in the room, including ceilings, walls, ventilation grilles, floors, furniture, and all patient care equipment. Low-touch and hidden surfaces are included, which distinguishes it from routine cleaning.
How long does terminal cleaning take?
Duration depends on room size and complexity, but the contact time for the disinfectant alone typically requires 10 minutes or more per surface application. Rushing contact time is the most common compliance failure in terminal cleaning procedures.
Is terminal cleaning the same as a deep clean?
No. "Deep clean" is a commercial term with no regulatory definition. Terminal cleaning is a regulated process with specific documentation, product registration, and sequence requirements enforced by The Joint Commission and QUAD A.
What records are required after terminal cleaning?
Records must include the disinfectant's product registration number, concentration, contact time, the name of the staff member who performed the clean, and a direct link to the trigger event. Incomplete records are rejected during accreditation surveys.